

In the first article in this series, I discussed the phenomenon of coral bleaching and how it can result in a pale or white-appearing coral. I also compared it to actual tissue loss in corals, showing how the two can resemble each other. In the second part, I covered a number of events, organisms, and conditions that could resemble both bleaching and coral disease, resulting in tissue loss or producing white areas on corals that are difficult to distinguish as to their cause. In this last article, I will treat the subject of the coral diseases known collectively as “White Syndromes” (Antonius 1995).
Coral diseases can be quite different in the gross appearance of the diseased organism. In some cases, the signs are fairly distinct, while in others they are so similar that there is no way to tell them apart. This becomes even more problematic given that the etiology or set of conditions that cause and factor into the disease condition, may not be well established or known at all. In numerous diseases, the pathological condition that is observed consists of an area of bleached tissue or an area of recent tissue loss so that the normally pigmented tissue presents a sharp contrast to the white recently exposed skeleton.
The area that borders the healthy tissue, including any degenerating tissue and, usually, the area of white exposed skeleton, is called the “band line.” The band line may be quite broad, or very narrow. It may make sense that a coral disease with a slow progression will generally have a narrow band line, since other flora and fauna, obscuring the white color soon overtake the white exposed skeleton. In contrast, a rapidly progressing disease typically has a wide band line as the tissue loss progresses quickly, leaving more skeleton exposed before flora and fauna can overgrow the exposed white skeleton.
In some cases, disease may result in bleaching, either locally or across areas of the colony. Conversely, bleaching can increase susceptibility to disease. In some diseases (for example, Yellow Blotch Disease), the band line may have bleached tissue and areas of exposed skeleton. This particular disease tends to move very slowly, and yet has a wide disease band. This is because of the bleached regions that can extend upwards of several inches into the tissue that still covers the skeleton. Thus, each instance of disease must be carefully considered and observed over time.
The band line is important in another way. The rate of progression of white syndromes may be partially diagnostic in distinguishing the type of disease present. For example, White Band Disease (WBD) tends to move fairly slowly across the coral surface, whereas White Plague Type II (WPII) tends to move quite rapidly. Therefore, measuring the rate of tissue loss and the width of the band line can help a potential investigator to determine which of these two grossly similar diseases may be at work.
Becoming Familiar with the White Syndromes
There has been an increase in the reports of coral diseases over the past twenty years. The first white syndrome identified was WBD (Gladfelter 1977). This was followed by White Plague in the same year (Dustan 1977). Since then, a host of other white pathologies have been reported. For many of these, the cause or causative agent has yet to be identified, or has been tentatively identified. It is not yet known for certain if some of these diseases are the same, or variations of, another condition. It is equally possible that different and as yet unnamed diseases are being lumped into categories of currently named diseases because of a lack of proper study. For most coral diseases, the state of knowledge is greatly lacking. This may be even truer of the white syndromes. A table of currently named diseases with signs of white or somewhat white (pale) areas, and summarizing information about them, is shown below (Table 1). A photo gallery of some of the white syndromes is provided at the end of the article (Appendix 1).
| Name | Causative Agent(s) | Reference | Description |
|---|---|---|---|
| C= Caribbean IP = Indo-Pacific RS = Red Sea | |||
| White Band Disease Type I (WBDI) | Unknown – possible role of gram negative ovoid bacterial bodies in tissues of some samples (Peters et al. 1983) | Gladfelter 1982 | 1. Location – C, IP, RS (see note below) |
| 2. Tissue Loss – 1/8 – 1/2″/day | |||
| 3. Bleaching – no | |||
| 4. Band Width – 2-3″ | |||
| 5. Contagious – no | |||
| White Band Disease Type II (WBDII) | Vibrio carchariae – Questionable identification | Ritchie and Smith 1995 | 1. C |
| 2. up to 9cm/day | |||
| 3. yes – 5-10cm wide | |||
| 4. 2-3″ | |||
| 5. no | |||
| White Plague (WP) | Unknown | Dustan 1977 | 1. C, IP, RS |
| 2. “few mm/day” | |||
| 3. no | |||
| 4. few mm or less | |||
| 5. yes | |||
| White Plague Type II (WPII) | Sphingomonas sp. limited sampling | Zorpette 1995 | 1. C |
| 2. 1-10 cm/week | |||
| 3. no | |||
| 4. few mm or less | |||
| 5. yes | |||
| White Plague Type III (WPIII) | Unknown | Richardson and Aronson 2002 | 1. C |
| 2. 1-10cm/day | |||
| 3. no | |||
| 4. few mm or less | |||
| 5. yes | |||
| Patchy Necrosis | In submission (Santavy et al.), fecal deposition | Bruckner and Bruckner 1997 | 1. C – only A. palmata? |
| 2. 1-2 cm/day | |||
| 3. no | |||
| 4. few mm or less | |||
| 5. unk | |||
| Ulcerative White Spot Disease | In press – Vibrio and virus possible | Raymundo and Harvell 2000 | 1. IP – only Porites sp.? |
| 2. slow coalescence | |||
| 3. sometimes | |||
| 4. 3-5 mm round multifocal lesions | |||
| 5. yes | |||
| Shut Down Reaction (SDR) | Unknown | Antonius 1977 | 1. C, IP, RS |
| 2. to 10cm/hour or more | |||
| 3. no | |||
| 4. few mm or less | |||
| 5. yes | |||
| White Pox | In submission (Patterson et al.) | Porter 1996 | 1. C |
| 2. unknown – “fast” | |||
| 3. no | |||
| 4. not reported | |||
| 5. not reported | |||
| Yellow Blotch Disease | Unknown | Reeves 1994 | 1. C |
| 2. 7-15cm/year | |||
| 3. yes | |||
| 4. 2-10 cm | |||
| 5. no | |||
| Hyperplasia | Unknown | Loya et al. 1984 | 1. C, IP, RS |
| 2. not reported – very slow | |||
| 3. yes | |||
| 4. na | |||
| 5. no | |||
| Neoplasia | Unknown | Peters et al. 1986 | 1. C, IP, RS |
| 2. not reported – slow | |||
| 3. yes | |||
| 4. 1-20cm | |||
| 5. unk, probably not | |||
| Coccidium infection | Apicomplexa | Upton and Peters 1986 | 1. C |
| 2. not reported | |||
| 3. yes | |||
| 4. up to 4 x 5 cm | |||
| 5. yes | |||
| Stress Related Necrosis | No obvious pathogens | Peters 1984 | 1. C, IP, RS |
| 2. see WBD I | |||
| 3. see WBD I | |||
| 4. see WBD I | |||
| 5. see WBD I | |||
| Blistering Necrosis | Unknown | Peters 1984 | 1. unk. |
| 2. unk. | |||
| 3. unk. | |||
| 4. unk. | |||
| 5. unk. | |||
| Ring disease | Unknown | Weil 2001 | 1. unk. |
| 2. unk. | |||
| 3. unk. | |||
| 4. unk. | |||
| 5. unk. | |||
| Finger coral denuding syndrome | Unknown | Williams and Bunkley-Williams 2000 | 1. unk. |
| 2. unk. | |||
| 3. unk. | |||
| 4. unk. | |||
| 5. unk. | |||
| Star coral polyp necrosis | Unknown | Williams and Bunkley-Williams 2000 | 1. unk. |
| 2. unk. | |||
| 3. unk. | |||
| 4. unk. | |||
| 5. unk. | |||
| Skeletal Eroding Band | Halofolliculina corallasia | Antonius 1999 | 1. IP |
| 2. not reported | |||
| 3. no | |||
| 4. up to several cm | |||
| 5. not reported | |||
| Bacterial Bleaching | Vibrio shiloi Well characterized | Kushmaro 1996 | 1. Mediterranean |
| 2. approx. 0-30% bleached /week, temp dependent | |||
| 3. yes | |||
| 4. not applicable | |||
| 5. yes | |||
| Bacterial Lysis | Vibrio coralyticus recent discovery | Ben-Haim and Rosenberg 2002 | 1. IP |
| 2. est. up to several cm/day | |||
| 3. yes | |||
| 4. not reported | |||
| 5. yes | |||
In some of the diseases, one or more white “lines” indicating a band line may occur across a coral surface or around a colony or branch. Others appear as spots or patches on the coral surface, with the band line moving outward from a central focus or initiation point. In others, the result is bleaching or even colony-wide tissue release.
Factors in White Syndromes
Because so little is known about the cause and pathology of the many diseases, it is difficult to determine what the primary or secondary causes might be, including the influences of various stressors. In particular, there is a great deal of question as to the roles of pathogens and other biotic factors versus environmental stressors (abiotic factors). There is probably significant interaction between numerous factors to produce a disease condition. In seems to be a general consensus that for most coral disease, new pathogens never before seen are not to blame. Rather, the microbial ecology of corals is coming under study, and research is needed to determine various things; including whether pathogens are direct pathogens, opportunists, or normally associated with corals but causing disease because of chronic or acute stress to a habitat or individual coral colony. For at least one disease (bacterial bleaching), increasing temperature results in virulence genes getting “turned on” and resulting in pathogenicity. For at least four others — stress related necrosis, SDR, neoplasia, and hyperplasia — pathogens do not appear to be required at all, although further study is required.
There have been a number of attempts, though by no means exhaustive, to determine the role of other variables in coral disease. In particular, the role of coastal nutrients and effluxes have been examined to determine if a role exists between the reports of coral disease and the degree of nearness of affected sites to the coast. Similarly, studies have attempted to establish a correlation between variables such as season and temperature, with mixed results. Chemical and thermal effluents have been shown to play a role in several diseases, although it is not determined if the disease was attributed to the influence itself through direct toxicity or killing. Doldrums, or periods of low water movement have also been implicated in increased incidence of coral disease, as well as damage from storms. Bleaching has been suggested to increase the susceptibility of corals to disease. Other biotic factors have been suggested in increasing or decreasing susceptibility to coral disease, including the presence or absence of commensal crabs, predation by snails, fishes, and sea stars, and the deposition of fecal material by fish and sediments by coastal efflux or storms.
White Syndromes in Aquarium Corals
Most of the research in coral disease has been done in the Caribbean. This is also the area where the greatest effect of coral diseases has been seen on wild populations. The Red Sea, also highly impacted by various stresses, runs a distant second in terms of study. More recently, areas in the Philippines and the Great Barrier Reef in Australia have begun reporting increased numbers and types of coral diseases. It is probably likely that more study from this vast region will be forthcoming. As a consequence, however, the relation of coral disease to aquarium corals is difficult since most aquarium corals are not Atlantic or Caribbean species. Coupled with the relative lack of knowledge of the disease, the difficulty of diagnosing a particular disease, especially the white syndromes, may be impractical to impossible for the aquarist. It is my impression that the majority of problems that result in signs of whitening on aquarium corals are not diseases. Of those that are diseases, Shut Down Reaction (this is called RTN by aquarists) is unquestionably the most common, yet appears to be one of the least common in the wild. I have also seen and experienced many cases of what would appear to be bacterial bleaching and WBD, although the actual diagnosis is unconfirmed in all cases. This is not only because studies have not been done to confirm the diagnosis, but also because we don’t yet know what causes the disease.
Treatment
Unfortunately, because the causative agents are not known, and because diagnosing a disease is so difficult, treatment protocols are extremely limited and experimental. For conditions that show signs of a slowly progressing white band line, there are several possible options. The first is fragmentation. Often, conditions that do not seem to allow for the health of a colony prove adequate for smaller fragments. If there is an associated pathogen, fragmentation well into healthy tissue may remove that element. Of course, fragmentation involves both injury and stress. Conditions should be optimal for the resulting fragment, and I feel that areas of exposed tissue should be sealed as in the following method described.
The second treatment method is sealing the affected area. Use of adhesives to seal a disease band has resulted in successful trials in the aquarium and in the wild. Epoxy putty or superglue can be applied across the entire disease band and into healthy tissue. This seems to result in stopping disease progression in many cases. It is important to completely seal the band, leaving no exposed areas or “gaps.” Epoxy putty must be pressed firmly down onto the coral surface to ensure a good seal. Superglue has been used as a field dressing for cuts and wounds, and it can stick to moist and slippery surfaces. As such, I find that, where applicable, it is superior to epoxy putty for sealing tissue. In light of my comments above, I feel that coral fragments should have their broken and exposed ends well sealed with superglue as a prophylactic method. I think this is even the case in the course of normal fragmentation for asexual propagation to reduce the risk of potential infection.
A third treatment method that I find to often halt disease progression with many white syndromes is isolation. I have found remarkable success in simply removing an affected colony to a quarantine tank with strong water flow and newly made seawater. I would rather not speculate on the rationale or potential reasons for its effectiveness, but it is impressively successful. Once the band line has stopped its progression, and the coral appear healthy or has begun growing or recovering exposed skeleton, it can generally be moved back to the display tank without incident.
As for using medications, antibiotics, and other substances as treatments, I would refer interested parties to protocols outlined in Borneman (2001) and Borneman (2002). I strongly caution against the use of antibiotics to treat corals blindly or as a prophylactic measure. I urge anyone so inclined to use such experimental protocols only after exhausting other methods, to use great care in the exposure of anything other than the affected coral to antibiotics, and to take great pains in the proper disposal of treatment water following the treatment regimen. I would also urge those so inclined to keep careful records on the protocol and its results, documenting as much as possible, and reporting the results to ensure that such trials have value. I would be happy to act as the recipient for such records.
Conclusion
Within this series, I have explained how the appearance of pale or white areas on coral can be the result of either bleaching or tissue loss. Bleaching is perhaps the most easily determined since living tissue remains on the coral. Tissue loss that results in exposed skeleton can be caused by many factors including mechanical abrasion or injury, predation, starvation (recession), chemical toxicity, and disease. Coral disease is often attributed as a cause of tissue loss when it may be more likely that other factors are involved or are causative. Even if coral disease is a factor in tissue loss, the relative state of knowledge of these conditions makes it very difficult to ascertain the identification, cause or solution to the disease. Each case requires careful observation and consideration. A systematic approach that addresses all potential factors and variables is probably an aquarist’s best method to determining what is happening, and in providing a solution that minimizes or halts any further loss of the integrity of the colony, as a whole.
I welcome inquiries into further reference material for any of the statements or information provided in this article.
References
- Antonius A. 1999. “Halofolliculina corallasia, a new coral-killing ciliate on Indo-Pacific reefs.” Coral Reefs 18: 300.
- Antonius A. 1995. “Pathologic syndromes on reef corals: a review.” Proc 2nd Eur Meet ISRS. Pub Serv Geol Lux 29: 231-235.
- Antonius A. 1977. “Coral mortality in reefs: a problem for science and management.” Proc 3rd Int Coral Reef Symp 1: 617-23.
- Ben-Haim Y, Rosenberg E. 2002. “A novel Vibrio sp. pathogen of the coral Pocillopora damicornis.” Mar Biol, online edition. http://link.springer.de/link/service/journals/00227/contents/02/00797
- Borneman EH. 2001. Aquarium Corals. Microcosm/TFH, neptune City. 464 pp.
- Borneman EH. 2002. “Bacterial infections: a response to recent “reef notes” columns.” Reefkeeping 1(4). http://www.reefkeeping.com
- Bruckner AW, Bruckner RJ. 1997. “Outbreak of coral disease in Puerto Rico.” Coral Reefs 16: 260.
- Dustan P. 1977. “Vitality of reef coral populations off Key Largo, Florida: recruitment and mortality.” Env Geol. 2: 51-8.
- Glabfelter WB 1982. “White-band disease in Acropora palmata: implications for the structure and growth of shallow reefs.” Bull Mar Sci 32: 639-43.
- Gladfelter WB, Gladfelter EH, Monohan RK, Ogden JC. 1977. “Environmental studies of Buck Island Reef National Monument, St. Croix, US Virgin Islands.” Spec Rep Natl Park Serv, US Dept Interior. 173 pp.
- Kushmaro A, Loya Y, Fine M, Rosenberg E. 1996. “Bacterial infection and coral bleaching.” Nature 380: 396.
- Loya Y, Bull G, Pichon M. 1984. “Tumor formation in scleractinian corals.” Helgo wiss Meers 37: 99-112.
- Peters EC. 1992. “The role of environmental stress in the development of coral diseases and micro-parasite infestations.” Amer Zool 32: 960.
- Peters EC, Halas JC, McCarty HBJ. 1986. “Calicoblastic neoplasms in Acropora palmata, with a review of reports on anomalies of growth and form in corals.” J Natl Cancer Inst 76: 895-912.
- Peters EC. 1984. “A survey of cellular reactions to environmental stress and disease in Caribbean scleractinian corals.” Helgo wiss Meer 37: 113-37.
- Peters EC, Oprandy JJ, Yevich PP. 1983. “Possible causal agent of “White Band Disease” in Caribbean acroporid corals.” J Inv Path 41: 394-6.
- Porter JW, Meier OW. 1992. “Quantification of loss and change in Floridian reef coral populations.” Amer Zool 23: 625-640.
- Raymundo LJH, Harvell CD. In press. “Porites Ulcerative White Spot Disease: a new disease impacting Indo-Pacific coral reefs.”
- Reeves L. 1994. “Newly discovered: Yellow band disease strikes Keys reefs.” Underwater USA 11: 16.
- Richardson LL, Aronson RA. In press. “Infectious diseases of reef corals. Proc 9th Int Coral Reef Symp, Bali.”
- Ritchie KB, Smith GW. 1995. “Preferential carbon utilization by surface bacterial communities from water mass, normal, and white-band diseased Acropora cervicornis.” Mol Mar Biol Biotech 4: 345-52.
- Upton SJ, Peters EC. 1986. “A new and unusual species of coccidium Apicomplexa: Agamococcidiorida from Caribbean scleractinian corals.” J Invert Path 47:184-93.
- Weil E. 2001. “Caribbean coral reef diseases: status and research needs. In: Priorities for Caribbean Coral Research” (McManus J, ed.) Proceedings, Miami: 1-8.
- Williams EH Jr., Bunkley-Williams, L. 2000. “Marine major ecological disturbances of the Caribbean.” Infect Dis Rev 2: 110-127.
- Zorpette G. 1995. “More coral trouble.” Sci Amer 273: 37-8.
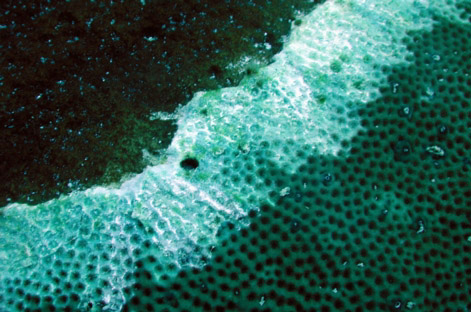
Appendix 1: Reference Photos

White Band Disease in Acropora palmata (wild)
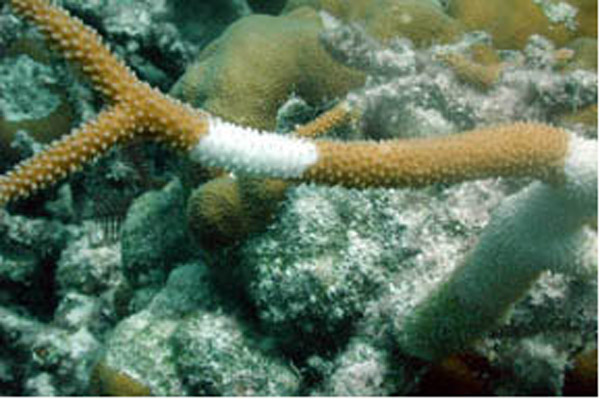
White Band Disease in Acropora cervicornis (wild)

White Plague Type II in Colpophyllia natans and Agaricia agaracites (wild)
Skeletal Eroding Band in Siderastrea siderea (wild)

Shut Down Reaction in Acropora cervicornis (wild)

Shut Down Reaction in Acropora sp. (aquarium)
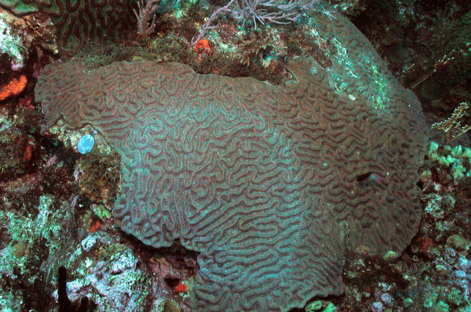
Ring Disease in Colpophyllia natans (wild)

Patchy necrosis in Acropora palmata (wild)

Neoplasm in Acropora palmata (wild)

Neoplasm in Acropora sp. (aquarium)

Possible bacterial bleaching in Goniopora sp. (wild)
0 Comments